Search Blog
Categories
Popular Blog
World Brain Day 2026: 7 Warning Signs of a Brain Tumour You Should Never Ignore
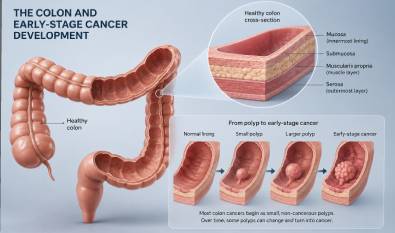
7 Warning Signs of Colon Cancer and Why Early Screening Saves Lives
Sarcoma Awareness Month 2026: The Forgotten Cancer That Deserves Your Attention
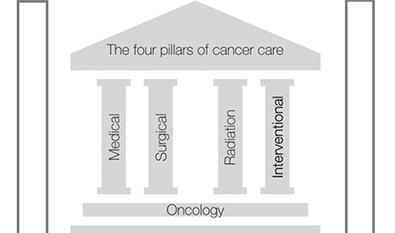
Interventional Radiology